-
Templates
1099 FormsAccurately report 1099 information returns and ensure IRS filing with easeExplore all templatesW-9 W-8 FormsEasily manage and share taxpayer details to streamline payments and meet IRS requirements with confidenceExplore all templatesOther Tax FormsFillable tax forms simplify and speed up your tax filing process and aid with recordkeeping.Explore all templatesReal EstateReal estate templates for all cases, from sale to rentals, save you a lot of time and effort.Explore all templatesLogisticsSimplify your trucking and logistics paperwork with our ready-to-use transportation and freight templates.Explore all templatesMedicalMedical forms help you keep patient documentation organized and secure.Explore all templatesBill of SaleBill of Sale templates streamline the transfer of ownership with clarity and protection.Explore all templatesContractsVarious contract templates ensure efficient and clear legal transactions.Explore all templatesEducationEducational forms and templates enhance the learning experience and student management.Explore all templates
-
Features
FeaturesAI-Enhanced Document Solutions for Contractor-Client Success and IRS ComplianceExplore all featuresAI Summarizer Check out the featureAI PDF summarizer makes your document workflow even faster. Ask AI to summarize PDF, assist you with tax forms, complete assignments, and more using just one tool.Sign PDF Check out the featurePDFLiner gives the opportunity to sign documents online, save them, send at once by email or print. Register now, upload your document and e-sign it onlineFill Out PDF Check out the featurePDFLiner provides different tools for filling in PDF forms. All you need is to register, upload the necessary document and start filling it out.Draw on a PDF Check out the featureDraw lines, circles, and other drawings on PDF using tools of PDFLiner online. Streamline your document editing process, speeding up your productivity
- Solutions
- Features
- Blog
- Support
- Pricing
- Log in
- Sign Up





























































Healthcare Templates
-
 Doctor Note for Work
What Is Doctor Note for Work
Fillable doctors note also known as doctor’s excuse letter is the form that is provided by the doctor to the patient whenever it is required by the employer. It is an official document that explains a day or several days
Doctor Note for Work
What Is Doctor Note for Work
Fillable doctors note also known as doctor’s excuse letter is the form that is provided by the doctor to the patient whenever it is required by the employer. It is an official document that explains a day or several days
-
 Doctor Return to Work Note
What Is a Return to Work Note From a Doctor?
Doctor Return to Work Note is a form that confirms or disclaims your ability to get back to work after some time that you were absent because of your health status. It also points to some physical restrictions
Doctor Return to Work Note
What Is a Return to Work Note From a Doctor?
Doctor Return to Work Note is a form that confirms or disclaims your ability to get back to work after some time that you were absent because of your health status. It also points to some physical restrictions
-
 Patient Wristband Template
What Is a Patient Wristband Template?
A patient wristband template is a fillable blank form to be used when generating an informative wristband for inpatients. The primary purpose of this form is to make essential medical information visible.
W
Patient Wristband Template
What Is a Patient Wristband Template?
A patient wristband template is a fillable blank form to be used when generating an informative wristband for inpatients. The primary purpose of this form is to make essential medical information visible.
W
-
 Prisma Health Doctors Note Form
What Is a Prisma Health Doctors Note
The Prisma Health Doctor's Note is an official medical document issued by healthcare specialists affiliated with Prisma Health. Its primary purpose is to provide a formal and legitimate record of a patient's me
Prisma Health Doctors Note Form
What Is a Prisma Health Doctors Note
The Prisma Health Doctor's Note is an official medical document issued by healthcare specialists affiliated with Prisma Health. Its primary purpose is to provide a formal and legitimate record of a patient's me
-
 Miscarriage Doctor Note
What Is a Miscarriage Doctor’s Note?
A doctor's note about a miscarriage is a document that says a woman has had a miscarriage and needs time to recover. Certificate usually states how long the woman needs to recover and may offer other recommen
Miscarriage Doctor Note
What Is a Miscarriage Doctor’s Note?
A doctor's note about a miscarriage is a document that says a woman has had a miscarriage and needs time to recover. Certificate usually states how long the woman needs to recover and may offer other recommen
-
 COVID-19 Doctor Note
What Is COVID-19 Doctor Note Template?
Covid-19 doctor note template is also called a letter from a Health Care professional supporting workplace requests for accommodations related to COVID-19. This is the document that suggests you need to stay at home
COVID-19 Doctor Note
What Is COVID-19 Doctor Note Template?
Covid-19 doctor note template is also called a letter from a Health Care professional supporting workplace requests for accommodations related to COVID-19. This is the document that suggests you need to stay at home
-
 STD Testing Results Form
What Is an STD Testing Results Form?
The printable blank STD test result form is used to protect your health by diagnosing venereal diseases. Sexually transmitted diseases (STDs) can be conveyed through any sexual activity. This specific PDF for
STD Testing Results Form
What Is an STD Testing Results Form?
The printable blank STD test result form is used to protect your health by diagnosing venereal diseases. Sexually transmitted diseases (STDs) can be conveyed through any sexual activity. This specific PDF for
-
 PMRF Form
What is a PMRF Form
The PMRF Form of PhilHealth is a two-page application that Filipino citizens can use to become a member of the local insurance program. You need to obtain a PhilHealth Identification Number before filling it out. You do not need other
PMRF Form
What is a PMRF Form
The PMRF Form of PhilHealth is a two-page application that Filipino citizens can use to become a member of the local insurance program. You need to obtain a PhilHealth Identification Number before filling it out. You do not need other
-
 Proof of Vaccination Form
What Is Pet Vaccination Form?
Proof of vaccination form for pets is a federal veterinary form of the US that is designed to provide approval of vaccination of an animal if it is requested by any private or federal institution. Dog Vaccination Record
Proof of Vaccination Form
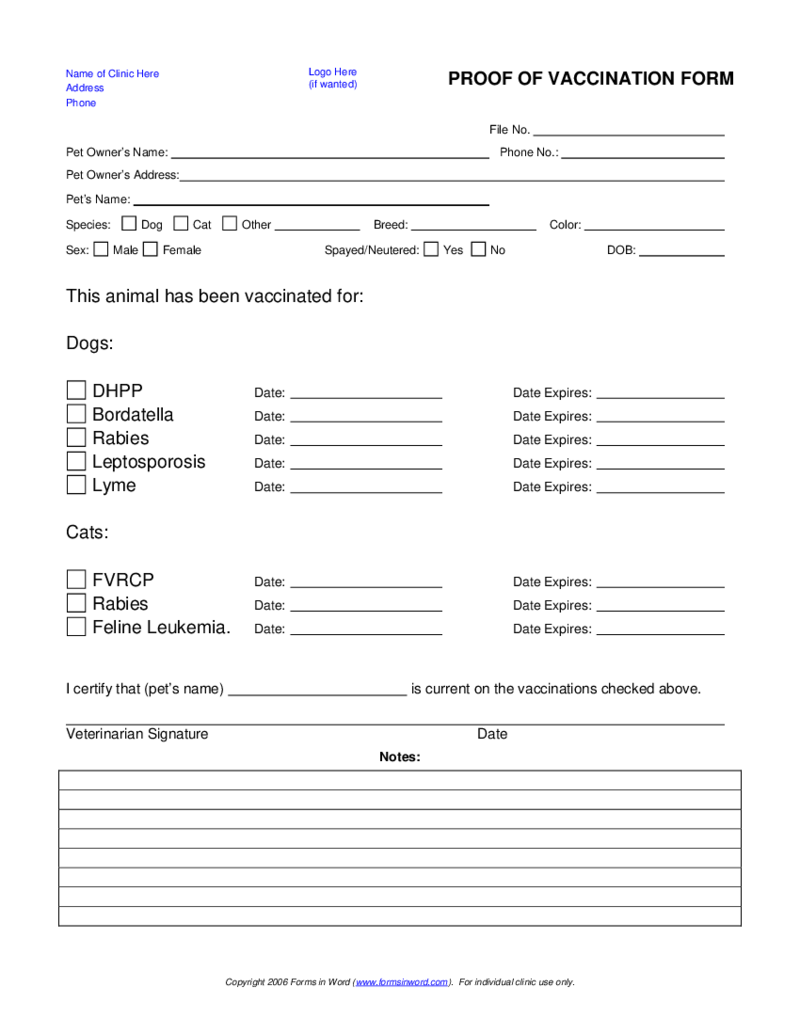
What Is Pet Vaccination Form?
Proof of vaccination form for pets is a federal veterinary form of the US that is designed to provide approval of vaccination of an animal if it is requested by any private or federal institution. Dog Vaccination Record
-
 Medicare enrolment form (MS004)
What Is Medicare Enrolment Form MS004
It’s a document designed to facilitate enrollment in the Medicare program, Australia's national healthcare system. Its purpose is to collect vital information from individuals seeking Medicare coverage, incl
Medicare enrolment form (MS004)
What Is Medicare Enrolment Form MS004
It’s a document designed to facilitate enrollment in the Medicare program, Australia's national healthcare system. Its purpose is to collect vital information from individuals seeking Medicare coverage, incl
-
 Emotional Support Animal Letter
What Is an Emotional Support Animal Letter
An Emotional Support Animal (ESA) Letter is a document issued by a mental health professional that verifies the therapeutic need for an emotional support pet. Its purpose is to grant individuals with emotional or
Emotional Support Animal Letter
What Is an Emotional Support Animal Letter
An Emotional Support Animal (ESA) Letter is a document issued by a mental health professional that verifies the therapeutic need for an emotional support pet. Its purpose is to grant individuals with emotional or
-
 Application for a Canada Pension Plan Retirement Pension
What Is ISP 1000 Form
Also known as Application for a Canada Pension Plan Retirement Pension, the ISP 1000 Form is an important document for individuals in Canada. Its fundamental purpose is to facilitate the application for the Canada Pension Plan (CPP)
Application for a Canada Pension Plan Retirement Pension
What Is ISP 1000 Form
Also known as Application for a Canada Pension Plan Retirement Pension, the ISP 1000 Form is an important document for individuals in Canada. Its fundamental purpose is to facilitate the application for the Canada Pension Plan (CPP)
What Are Healthcare Templates?
Healthcare templates are fillable forms required by patients, doctors, medical professionals, hospitals, private clinics, and other healthcare institutions. For a specialist, these templates make it easier to register new patients and examine their medical history. For a patient, they are a helpful tool to collect their personal information, general medical history, and contact data in case of an emergency. Using healthcare form templates, a medical professional can keep an eye on the patient's condition and progress of treatment.
The scope of use of such samples is wide. For example, an employer has to confirm or disclaim their ability to return to work after some time of their absence because of their health status. For this, a specialized form called a Return to Work Note From a Doctor is filled out. If you have a pet, a private or federal institution may ask you to complete a Proof of Vaccination Form for pets to ensure that it was vaccinated.
Most Popular Healthcare Form Templates
Whether you are a doctor looking for a customizable blank for your clinic or a patient who needs to provide their medical history and test results in a standardized format, the templates below can help you cover the task. Here is a list of the most popular medical forms:
- Personal Health Record Template
The first blank is called a Personal Health Record Template (or simply PHR) used by a patient to store and track their health information. It can help you monitor your healthcare providers, treatments, and appointments. If you have a personal medical record template, you are empowered to make informed decisions about your healthcare and monitor important health information. - COVID-19 Doctor Note
Nowadays, this healthcare template is highly in-demand. This document states that a person needs to stay at home for 14 working days because of illness. This form is given to a person by a professional physician. This form is essential to isolate the ill employee from other workers and clients. This document lists symptoms based on the health problems of a patient which are further certified by a medical specialist. This way, a professional ensures that the employee can be contagious if they attend work soon. - Patient Wristband Template
This blank is needed to make an informative wristband for a patient. It enables essential medical data to be visible. A medical worker might be in charge of filling out a Patient Wristband Form on admission. A patient might need to wear a special wristband when they are in a clinic or a hospital. Since the form’s design was built to report crucial patient data, it is very short, so it won’t take you long to complete it. - Proof of Vaccination Form
A Proof of Vaccination Form is required for traveling with a pet to take it through control and cross the border. It is suitable only for dogs and cats. It contains information about vaccinations such as DHPP, Bordetella, Rabies, Lyme, and Leptospirosis (for dogs) and FVRCP, Rabies, and Feline Leukemia (for cats). It’s essential to ensure that the timeframe of your journey corresponds with the expiry dates of vaccines. The Proof of Vaccination Form may be required by Airport and Land border control services, veterinarian clinics, animal exhibitions, etc. - Dental Excuse Note
A Dental Excuse Note Form is used by a dentist who wants to notify a school about the appointment with a student and how long a medical procedure will last. Since it is not a business agreement, the document does not require legal bounding. It enables schools, teachers, parents, and students to ensure their day off is legal. A fillable Dental Excuse Note is available in any dental clinic. It includes such data as the date, the name of a student who wants an excuse from the studies, the time of appointment at the medical office, the end of the appointment, for how many days the student must be excused from studies, the date they will return to school, and the doctor’s name.
Where to Get Healthcare Services Online Templates
These templates are available online, and you can get them on the official website of a healthcare provider. However, sometimes, you might not find a suitable template there. This is where you can address PDFLiner, a versatile online platform for editing various PDF documents. It offers a rich library of ready-made templates, which saves lots of time seeking and filling out a needed form. This solution can also help you significantly minimize your paper consumption since you can send the downloaded PDF electronically. It helps you to protect your sensitive data due to secure connection, draw, highlight, erase the text, create fillable fields on any template, and even sign the form digitally.